It’s not a matter of if, but when a
What is MF with Thrombocytopenia?
MF is a rare bone marrow cancer. It is part of a related group of blood cancers known as myeloproliferative neoplasms. MF can occur on its own, called primary myelofibrosis, or as a progression of polycythemia vera and essential thrombocythemia. The cancer develops when a mutation occurs in the DNA of a single hematopoietic stem cell. Over time, abnormal cell production overtakes the bone marrow’s ability to produce enough normal blood cells, which leads to formation of fibrous scar tissue.2
MF with thrombocytopenia can be a challenge to treat as the disease accelerates and becomes more complicated, thus causing worsening symptoms.1,3
Thrombocytopenia can be seen at myelofibrosis diagnosis and can become more prevalent over time.1,3,4
~25% are already thrombocytopenic at presentation3*
~70% will be thrombocytopenic at some
point in their MF story4†
- *In a retrospective cohort analysis (1984-2015) of 1269 patients with MF and thrombocytopenia, 25% had moderate to severe thrombocytopenia (plt ≤100 x 109/L).3
- †Based on a retrospective study of 807 physicians from 12 countries (60% EU, 25% US, 15% ex-US/EU) who completed surveys between April 2017 to June 2018, 54% from academic centers and 46% from community-based centers. There were approximately 18,000 patients with MF in the US and 24,000 in the EU.4
DATA FROM A PROSPECTIVE ANALYSIS
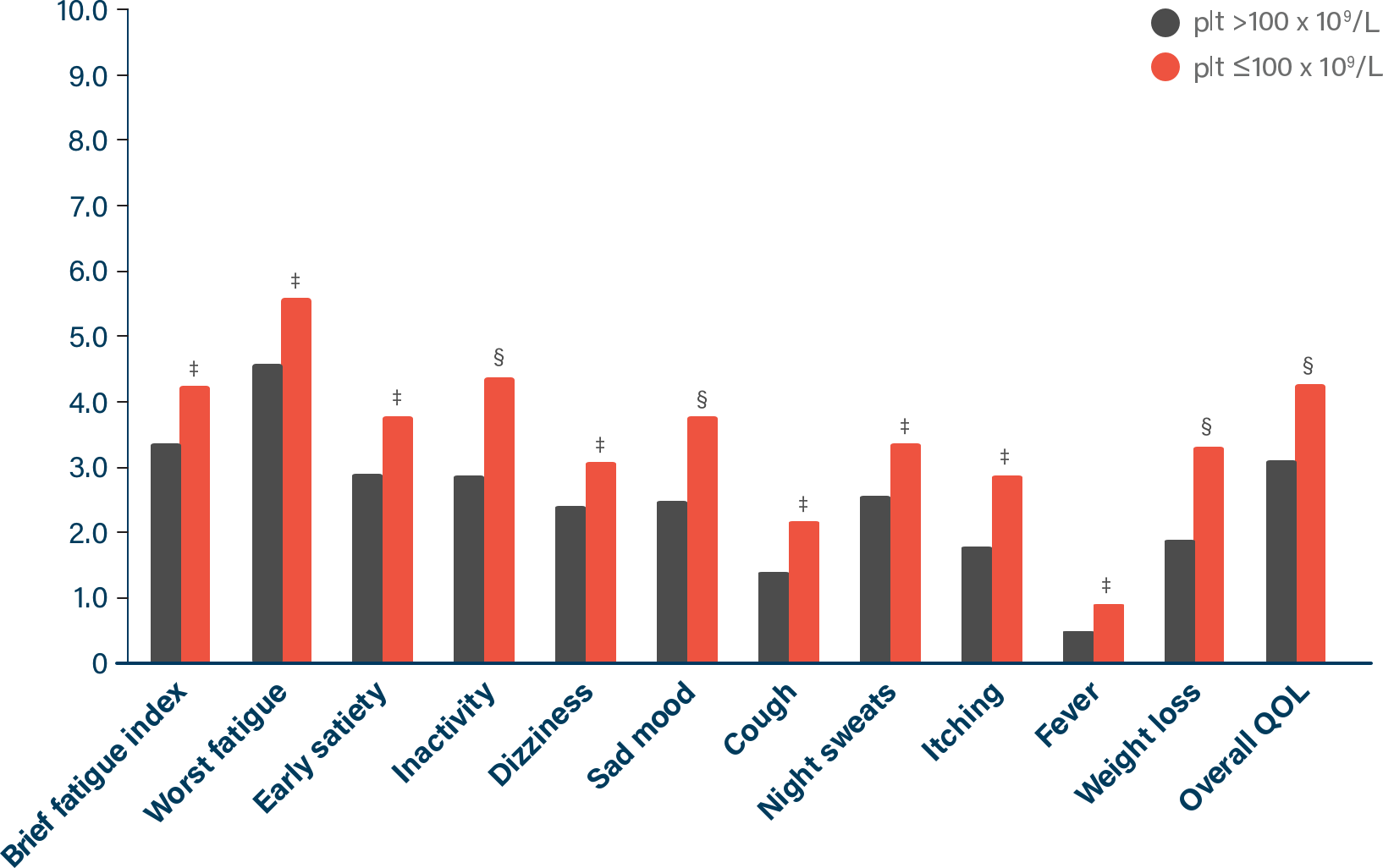
Patients with thrombocytopenia experienced significantly worse symptom burden than patients without it5‡
Image
Image
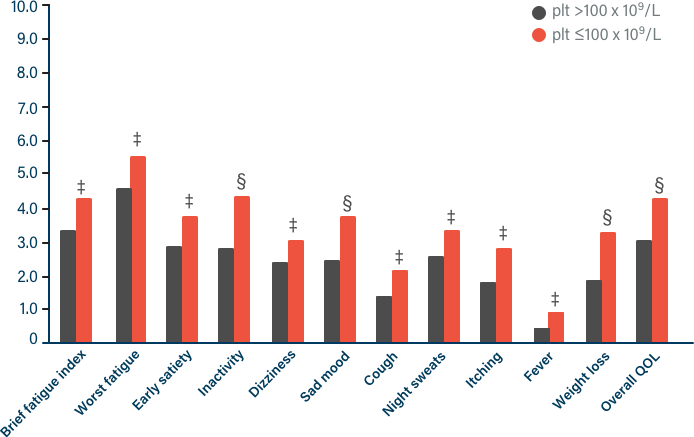
Adapted from Scotch AH, et al. 2017.
- ‡This was an observational, international, real-world study in which data were prospectively collected from 418 patients with MF (89 patients had thrombocytopenia, and 329 did not). Patients completed an MPN-SAF via self-reporting.5
- §P<0.05.
- ‖P<0.001.
How impactful is thrombocytopenia in MF?
MF with thrombocytopenia is a story associated with poor patient outcomes3¶
DATA FROM A RETROSPECTIVE COHORT ANALYSIS
As thrombocytopenia continued to worsen, overall survival (OS) became significantly reduced
Platelets
Months (Median OS)
>100 x 109/L
57
≤100 x 109/L
26
As MF progresses, is it time to consider the next chapter of the story?
- ¶In a retrospective cohort analysis of 1269 patients who had MF with thrombocytopenia (1984-2015), patients with thrombocytopenia (plt ≤100 x 109/L) had significantly worse survival than those with normal platelet counts—with a 1.7-fold increased risk of death (26 vs 57 months, P<0.001, HR=1.7 [95% CI: 1.37-2]).
What could your patient’s symptoms be telling you about their myelofibrosis progression?
Worsening symptoms can give you another way to recognize when their disease is becoming a more aggressive challenge to manage.
Talking with patients about their myelofibrosis symptoms can tell you more about their disease progression1,6:
Image
Do they feel full (satiety) earlier than usual?
Image
Has there been any abdominal discomfort or pain under their left ribs?
Image
Are they feeling more tired or weaker than usual?
Image
Have they noticed any unusual bruising and/or bleeding?
Image

How can we help?
If you're looking to stay up to date on the latest news or would like to request a representative or field reimbursement manager, you can do it all in one place—in almost no time.
- CI=confidence interval; EU=European Union; HR=hazard ratio; MOA=mechanism of action; NCCN=National Comprehensive Cancer Network® (NCCN®); plt=platelet counts; QOL=quality of life; US=United States.
- References: 1. Vachhani P, et al. Expert Opin Pharmacother. 2023;24(8):901-912. 2. Marcellino BK, et al. Clin Lymphoma Myeloma Leuk. 2020;20(7):415-421. 3. Masarova L, et al. Eur J Haematol. 2018;100(3):257-263. 4. Masarova L, et al. Leuk Res. 2020;91:106338. 5. Scotch AH, et al. Leuk Res. 2017;63:34-40. 6. Leukemia & Lymphoma Society. Myelofibrosis facts. Revised April 2012. Accessed November 18, 2024. https://www.lls.org/sites/default/files/file_assets/FS14_Myelofibrosis_Fact%20Sheet_Final9.12.pdf
Previous